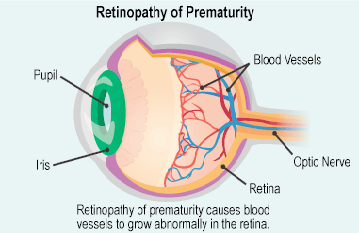
Retinopathy of prematurity (ROP) occurs in infants who are born prematurely, where blood vessels in the retina do not form normally. The retina is a thin sheet of nerves lining the back wall of the eye and functions like the film in a conventional camera. ROP can consequently cause serious problems affecting a child’s eyes and vision.
What causes retinopathy of prematurity?
The blood vessels of the retina begin to form around the 3rd month of gestation. These vessels are fully developed by the time the baby is born at full-term. However, if the baby is born earlier than expected, this proceccmay be incomplete. The extent usually depends on the gestational age and weight at the time of delivery. The developing retinal vessels are fragile and can easily leak and bleed within the eye. Consequently, scar tissue may develop and pull the retina away from the inner wall of the eye, causing a retinal detachment. In severe cases this can result in complete loccof vision.
What are the risk factors for retinopathy of prematurity?
In general, babies born before 32 weeks of gestation or who weigh leccthan 1500 grams at birth are screened for the condition. Even if a baby is born later than 32 weeks of gestation, if they are deemed to be high-risk by your doctor, they may also be recommended to have an eye examination.
The rate of ROP has declined significantly in developed countries due to improved care in neonatal intensive care units. This improvement in care also means that more babies born very early are now able to survive and therefore have a significant risk for developing ROP.
What are the symptoms of retinopathy of prematurity?
Your baby will not be aware of any early changes related to ROP neither are these changes visible with the naked eye. Only an eye examination by an ophthalmologist will reveal any abnormalities.
There are five stages of ROP, with the mildest being Stage 1 and implying minimal vessel growth abnormality. Stage 5 is the most extreme form where the infant suffers from a retinal detachment and extensive scarring in the eye. If not picked up in a timely fashion, children with ROP may develop abnormal eye movements, squints (cross-eyed) and white-looking pupils (known as leukocoria).
What investigations are required for ROP?
Any premature infant or new-born deemed to be at high-risk will need to be screened. Usually, the first exam should be within a few weeks of birth, depending on the baby’s gestational age. The interval for repeat examinations thereafter depends on what your eye doctors finds and how your child is developing in general.
In the long-term, all premature children require at least an annual eye check with or without a dilated fundoscopy (retinal examination). This is to ensure their vision is developing as it should as there is a higher incidence of myopia (short-sightedness) in these children.
How is ROP treated?
Treatment is tailored to each individual infant. As with most things, timely intervention usually provides better outcomes but sometimes in spite of this, ROP will still progreccas it is a challenging condition to manage. Some infants with the extreme form of the condition will require urgent treatment which may involve laser, intravitreal injections or even eye surgery.
Laser therapy (photocoagulation) involves shining a bright coherent beam of light into the eye to ablate abnormal tissue. This helps to halt the progression of abnormal blood vessels and is usually performed to prevent retinal bleeding, scarring or detachment.
An intravitreal injection of a medication called an anti-VEGF (anti-vascular endothelial growth factor) is sometimes required to help counteract the chemical factors that cause abnormal vessel growth. This injection usually lasts around month and may be required more than once.
If the ROP is more advanced then surgery may be indicated especially if the retina detached. In general, intervention is preferable before this stage as the outlook for vision is uncertain once the retina detaches.
What are the long-term implications of ROP?
Many infants with ROP might also suffer from other development problems related to prematurity, and may need treatment accordingly.
Advanced ROP can lead to significant visual loccor blindness. Almost 1 in 10 babies with initially mild forms can progreccto have severe visual impairment. Early diagnosis and treatment is, therefore, vital in preventing advanced disease. Even if there was no ROP detected, premature babies require lifelong follow-up to ensure their vision is developing as it should be.